
If I need the short answer, it’s this: UV-C is usually the better fit for fast room turnover, while ozone is better when hidden surfaces and hard-to-reach spots matter more.
I’d sum up the article this way:
- Both tools are add-ons, not replacements, for manual cleaning
- UV-C works fast, but only where the light can hit
- Ozone reaches more of the room, including cracks, seams, and shaded areas
- UV-C allows immediate re-entry after the cycle ends
- Ozone needs aeration and safety checks before staff can return
- Spores like C. difficile are harder for UV-C
- Ozone can work well against bacteria, viruses, and spores, but room sealing and timing matter
- Hospitals may use both: UV-C for routine turnover, ozone for after-hours deep treatment
One reason this matters: healthcare-associated infections are linked to about 63,000 deaths per year in the U.S. So the choice is not just about killing germs. It’s also about safety, room downtime, and how the space is used.
UV-C vs. Ozone Disinfection in Hospitals: Key Differences at a Glance
Quick Comparison
| Criteria | UV-C | Ozone |
|---|---|---|
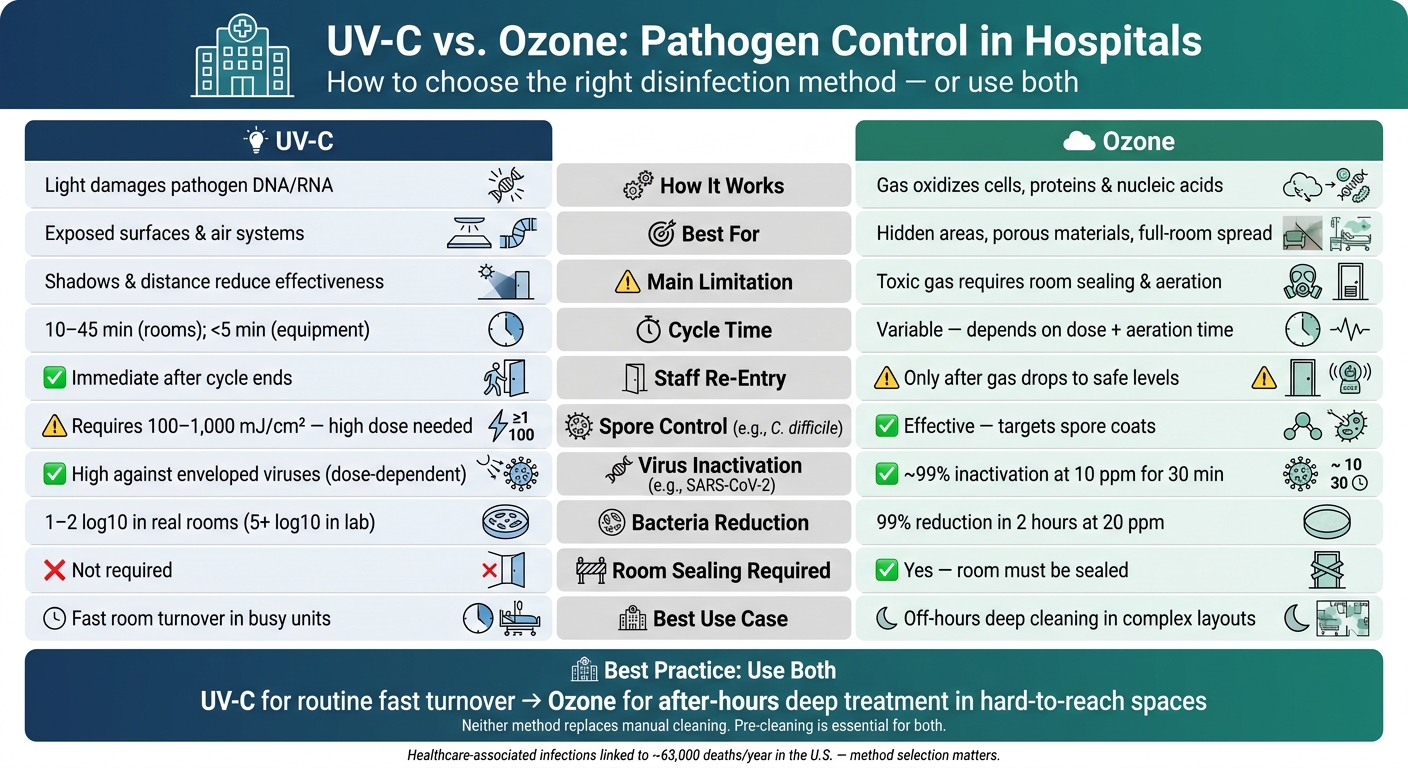
| How it works | Light damages DNA/RNA | Gas oxidizes cells, proteins, and nucleic acids |
| Best at | Exposed surfaces, air systems, short cycles | Hidden areas, porous materials, full-room spread |
| Main limit | Shadows and distance reduce effect | Toxic gas needs sealing, aeration, and checks |
| Re-entry | Right after cycle ends | Only after ozone drops to safe levels |
| Cycle time | Often 10–45 minutes for rooms | Changes by dose and aeration time |
| Spore control | Needs high dose | Often stronger option |
| Best use | Busy rooms needing fast reuse | Unoccupied spaces where full reach matters |
So if I were putting it in one line: choose UV-C for speed, ozone for reach, and both when one method leaves gaps.
sbb-itb-5fea4da
How Ozone and UV-C Perform Against Hospital Pathogens
The main issue isn’t whether ozone or UV-C can kill pathogens. It’s where each one works best in actual hospital use. That depends on the pathogen, the dose, exposure time, room layout, humidity, and how well the room was cleaned first.
Ozone: Strengths and Limits Against Pathogens
Ozone has one big edge: it moves as a gas, so it can reach shadowed spots and porous materials, including textiles and equipment surfaces. In one study, E. coli, E. faecalis, B. subtilis, and D. radiodurans were exposed to 20 ppm of ozone. The result was a major drop within 30 minutes, with up to 99% reduction in viable bacteria after 2 hours.
Ozone also does well against spore-forming organisms, including Bacillus subtilis. For viruses, the data is strong too. SARS-CoV-2 RNA showed major degradation after one hour of ozone exposure, and 10 ppm for 30 minutes is seen as a enough virucidal dose for 99% inactivation.
That said, ozone is not foolproof. Its results can slip when exposure time is too short, humidity shifts, or the space is not sealed well.
UV-C: Strengths and Limits Against Pathogens
UV-C works fast against vegetative bacteria and enveloped viruses when the dose is high enough. In lab conditions, UV-C LED devices produced reductions greater than 5 log10 for E. coli, S. aureus, and C. albicans. But hospitals are messier than labs, and that gap matters.
In actual hospital rooms, UV-C usually delivers 1 to 2 log10 reductions, mostly because equipment and room layout create shadows. Acinetobacter baumannii, for example, appears more resistant in day-to-day hospital use than lab results suggest. Spores are the hardest target. C. difficile and similar organisms need UV-C fluence of 100 to 1,000 mJ/cm², which is far above what vegetative bacteria need.
There’s also a physics problem. UV-C intensity falls fast with distance because of the inverse square law. Higher humidity can cut UV-C irradiance too.
So yes, UV-C is fast. But speed only helps when the light actually hits the surface.
Side-by-Side Comparison and Combined Results
The table below shows how both methods stack up by pathogen group, based on published hospital data.
| Pathogen Group | Ozone Performance | UV-C Performance | Key Notes |
|---|---|---|---|
| Gram-positive bacteria (e.g., MRSA) | High; 99% reduction in 2 hours at 20 ppm | High on exposed surfaces | Best on exposed surfaces; ozone covers shadowed areas |
| Gram-negative bacteria (e.g., E. coli, A. baumannii) | High; significant reduction within 30 minutes | High in lab; variable in real rooms | A. baumannii shows higher real-world resilience to UV-C |
| Spore-formers (e.g., C. difficile) | Effective; targets spore coats | Low; requires 100–1,000 mJ/cm² | Less reliable in cluttered rooms |
| Viruses (e.g., SARS-CoV-2) | High; degrades RNA and membrane receptors | High against enveloped viruses; dose-dependent | Ozone at 10 ppm for 30 minutes achieves ~99% viral inactivation |
| Fungi & yeasts (e.g., C. albicans) | Effective; disrupts cell walls | Moderate; requires higher doses than bacteria | UV-C LED achieved >5 log10 for C. albicans in lab conditions |
On paper, both tools look strong. In practice, the gap comes down to reach. UV-C is at its best on exposed surfaces. Ozone has more reach in hidden or porous areas, but it needs tighter control over exposure conditions. Similar results are seen when testing hydroxyl technology against pathogens, which offers another gas-phase alternative for complex environments.
Safety, Workflow, and Material Wear
Re-Entry Limits, Exposure Risks, and Staff Safety
Once a method works, the next test is simple: Can a hospital use it safely without slowing everything down? That’s where UV-C and ozone start to part ways, much like the differences between ozone and hydroxyl cleaning methods.
UV-C mainly puts the eyes and skin at risk. Ozone mainly affects the respiratory tract. Same goal, very different hazard profile.
Because ozone is toxic, treatment has to happen in unoccupied spaces. Staff can’t go back in until the facility confirms ozone levels have dropped to safe limits. That adds a step, and in a hospital, extra steps matter.
UV-C has its own risks too. Direct exposure to UV-C radiation can cause serious eye and skin damage. That’s why robotic UV-C systems use interlocks and motion sensors to prevent exposure. But once the cycle is over, there are no chemical residues, so staff can re-enter right away. In day-to-day operations, that’s a clear edge over ozone.
There’s one wrinkle worth calling out. UV-C lamps that emit wavelengths below 240 nm can generate ozone as a byproduct, which may call for extra safety steps even when the main goal is UV-C disinfection.
Cycle Time and Fit With Hospital Workflow
UV-C tends to fit better into fast hospital routines. Room cycles usually run 10 to 45 minutes, and small equipment cycles can take 25 seconds to 5 minutes. Ozone cycles are less fixed. They change based on the target concentration and the aeration time needed afterward.
Here’s how the workflow tradeoffs look side by side:
| Factor | UV-C | Ozone |
|---|---|---|
| Setup requirements | Position device; no sealing needed | Seal room; isolate HVAC |
| Treatment time | 10–45 min (rooms); <5 min (equipment) | Variable; depends on concentration and aeration |
| Ventilation after cycle | None; immediate re-entry | Required; must confirm safe levels before re-entry |
| Room sealing | Not required | Often necessary |
| HVAC considerations | Generally unaffected | Isolation typically required |
| Best fit | Faster room turnover | Longer cycles with re-entry verification |
For busy units working with tight turnover windows, UV-C is the more practical day-to-day option. Ozone makes more sense when a longer cycle and an aeration period won’t disrupt the schedule.
How Repeated Treatments Affect Materials and Equipment
Neither option is gentle on every material over time. With UV-C, the main issue is polymer degradation. Repeated exposure can discolor or weaken plastics and textiles if the total dose goes past material-specific thresholds. UV-C is also generally compatible with moisture-sensitive materials and equipment.
Ozone can wear down rubbers, plastics, and metals after repeated exposure. Hospitals should check material compatibility before making it part of routine use. That tradeoff feeds straight into the choice framework in the next section.
Choosing Ozone, UV-C, or Both: A Practical Framework
Performance and safety are already on the table. At this point, the decision is mostly about room access and how fast you need the space back. Match the method to the room itself: its shape, the pathogen you’re targeting, the time you have between uses, and whether people can stay out of the space.
When Ozone Is the Better Choice
Ozone makes the most sense when the room layout is the main problem. Since it’s a gas, it spreads through the full room volume and can reach behind furniture, into seams, and around equipment without needing a direct line of sight.
That said, ozone only works when the space can be fully unoccupied. You also need enough time for the gas to clear before anyone goes back in. If you can’t safely isolate and ventilate the space, ozone isn’t the better choice.
When turnover speed matters more than whole-room reach, UV-C usually fits better.
When UV-C Is the Better Choice
UV-C is a good fit for simpler room layouts where you can place the device in a way that limits shadows. Cycle times are faster – usually 10 to 45 minutes – and staff can re-enter right after the lamps switch off, which makes UV-C a better option for tight room turnovers.
To cut down on shadowing, use multi-position cycles and pair them with manual cleaning.
When one method handles what the other misses, run them together in sequence.
How to Run a Combined Ozone and UV-C Program
Some facilities get the best results by splitting the jobs between the two methods. UV-C can handle routine terminal cleaning during normal room turnover, while ozone can be saved for off-hours deep cleaning in rooms where layout or equipment density leaves gaps in UV-C coverage.
Conclusion: Key Tradeoffs Between Ozone and UV-C
In hospitals, the tradeoff comes down to four things: reach, speed, safety, and workflow. Ozone can get into hidden areas. UV-C works faster on exposed surfaces. That single gap shapes how hospitals use each method day to day.
Pre-cleaning still matters because debris can shield pathogens from both methods. If a surface is still dirty, neither option will do the job as well as it should.
After pre-cleaning, safety becomes the next limit. UV-C allows immediate re-entry once the lamps are off. Ozone, on the other hand, needs aeration before staff can safely return. This requirement is a standard part of ozone disinfection for event spaces and other large facilities to ensure occupant safety.
So the right choice depends on the pathogen, the room layout, the safety rules, and how much downtime the team can allow. In practice, the best programs match the method to the space and the moment: UV-C for fast turnover, ozone for harder-to-reach areas, and both when one method alone leaves gaps.
FAQs
Which option is better for C. diff rooms?
C. difficile spores are tough to kill. UV-C can cut contamination in some settings, but the results are mixed. Studies also show that adding UV-C to standard chlorine-based terminal cleaning does not clearly reduce contamination or the risk of transfer.
Ozone has a different role. It can treat unoccupied spaces and reach spots that are easy to miss during manual cleaning. But when it comes to C. difficile in particular, the evidence is still limited.
So while both methods may help in some situations, neither is broadly recommended on its own.
How much downtime does ozone add?
Ozone treatment only works when the space is empty. During the process, the gas is not safe for people or animals, so no one should be inside.
The treatment itself usually takes 30 to 120 minutes.
That’s only part of the timeline, though. You also need to account for downtime after treatment, while the ozone dissipates and the area is ventilated before anyone goes back in. Depending on the space and conditions, that extra wait can take 30 minutes to several hours.
Can hospitals safely use both together?
Yes. Hospitals can use UV-C and ozone together, and research suggests this combined approach can reduce pathogens in clinical settings.
UV-C is often used for surface and air disinfection. Ozone can help deal with broader contamination in a room. Put simply, UV-C targets exposed surfaces and air, while ozone can reach areas that are harder to clean by hand.
There’s one big catch: ozone must be used only in unoccupied spaces. That means safe use depends on strict safety protocols and professional handling.
Recent Comments